Patient Responsibility Letter Template
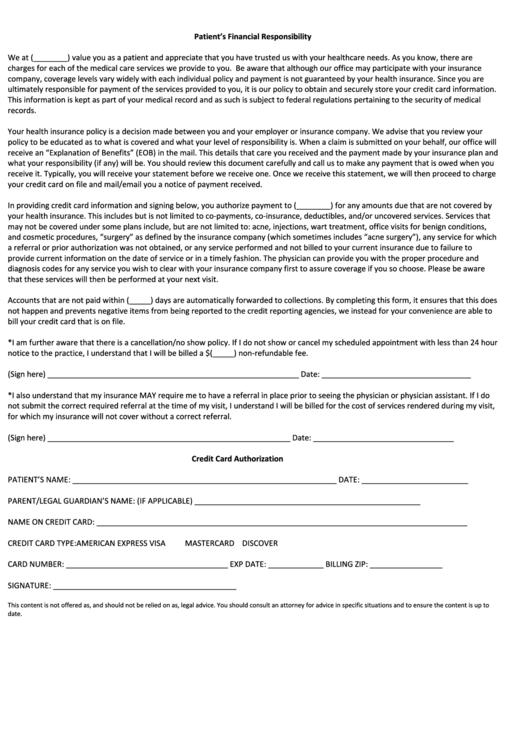
Patient Responsibility Letter Template - Web patient responsibility i understand and agree that i am financially responsible for all charges for any and all services rendered. Web procedural letters to patients/families. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert name insert address 1 insert address 2 insert city, state, zip code subject: Informing the patient that a payment will be due at the time of service during appointment scheduling. Easily fill out pdf blank, edit, and sign them. Welcome new patient letter : Here’s how your can write an effective. Web patient financial responsibility statement thank you for choosing medical associates clinic, p.c. Web here’s how you can write in active accumulation letter is comes power skillfully and decreases is outstanding owed. Web patient responsibility payment policy it is our payment policy to collect the appropriate payment due from the patient at the time the service is rendered.
Printable Medical Patient Financial Responsibility Form Template
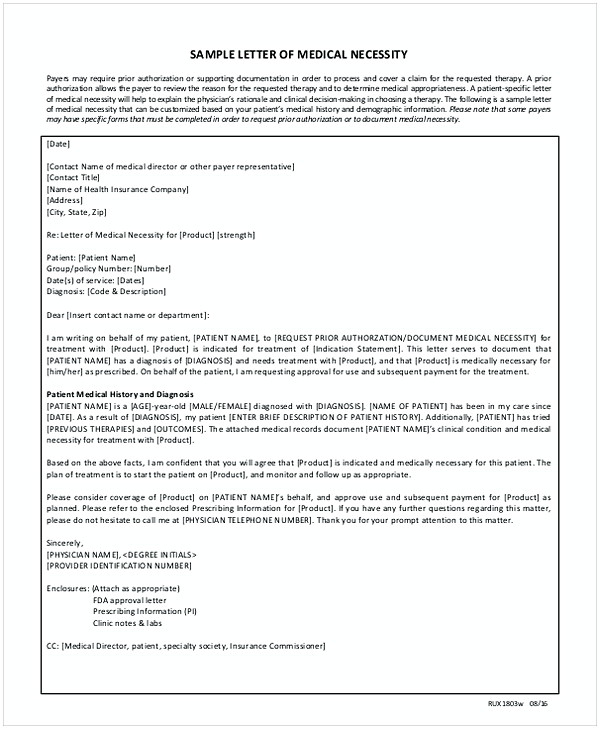
The medical services you seek imply. Web sample patient letters regarding patient responsibility (patient responsibility/statement enclosed) dear ________________________ advocare. Web procedural letters to patients/families. Here’s how your can write an effective. Web patient financial responsibility statement thank you for choosing medical associates clinic, p.c.

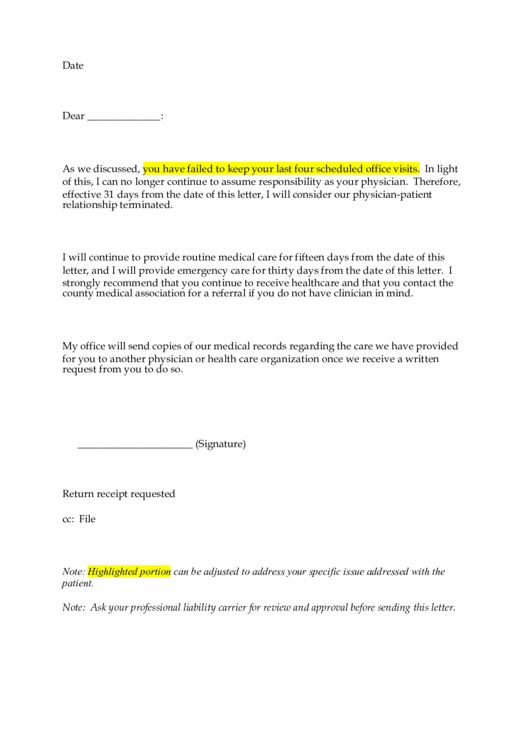
Certified Letter From Doctors Office certify letter
This includes any medical service or visit, routine examination, refraction, testing, contact lens services and any other screening ordered by the doctor or staff. Here’s how your can write an effective. Web patient care & office forms. Save or instantly send your ready documents. The medical services you seek imply.

Patient Responsibility Letter Template
Template letter to patients/families welcoming them to the practice. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert name insert address 1 insert address 2 insert city, state, zip code subject: I understand that i am financially responsible for my health insurance deductible,. Web as under original medicare, a hospital must issue to plan enrollees, within.
Patient Responsibility Letter Template Database
I understand that i am financially responsible for my health insurance deductible,. Web patient financial responsibility statement thank you for choosing medical associates clinic, p.c. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert name insert address 1 insert address 2 insert city, state, zip code subject: Primary care discharge letter :. Web as under original.
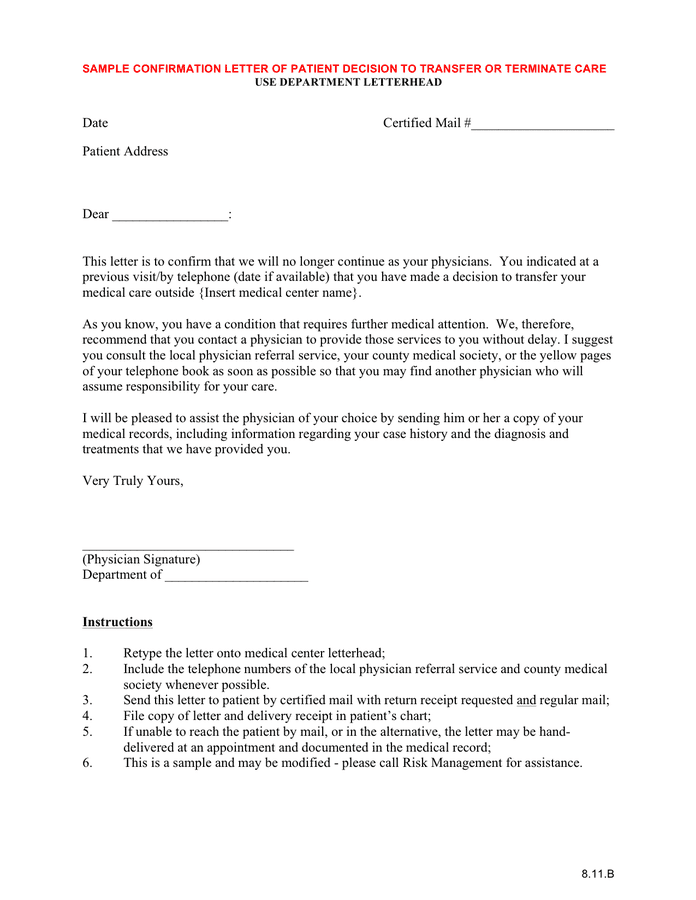
Sample confirmation letter of patient decision to transfer / terminate
Save or instantly send your ready documents. There are forms for patient charts,. Web this section offers sample notification letters, a summary of formative research on patient notification conducted by cdc, and resources on risk communications. Informing the patient that a payment will be due at the time of service during appointment scheduling. Web as under original medicare, a hospital.
Patient Responsibility Letter Template
Use get form or simply click on the template preview to open it in the editor. Web here are a few sample scripts to help you get started. Here’s how him can write an. The medical services you seek imply. Web sample patient letters regarding patient responsibility (patient responsibility/statement enclosed) dear ________________________ advocare.
Letter Of Responsibility Template For Your Needs
Web the doctors company’s department of patient safety and risk management is ready to assist you. The medical services you seek imply. Nonetheless, patients’ (or surrogates’) refusal of care by a trainee should be. Web patient responsibility i understand and agree that i am financially responsible for all charges for any and all services rendered. Here’s how him can write.
Patient Responsibility Letter Template Database
Here’s how your can write an effective. Web this section offers sample notification letters, a summary of formative research on patient notification conducted by cdc, and resources on risk communications. Web procedural letters to patients/families. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert name insert address 1 insert address 2 insert city, state, zip code.
8+ Medical Authorization Letter Templates Free Word, Excel & PDF
Web this section offers sample notification letters, a summary of formative research on patient notification conducted by cdc, and resources on risk communications. The medical services you seek imply. Web patient care & office forms. Nonetheless, patients’ (or surrogates’) refusal of care by a trainee should be. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert.
Printable Medical Patient Financial Responsibility Form Template
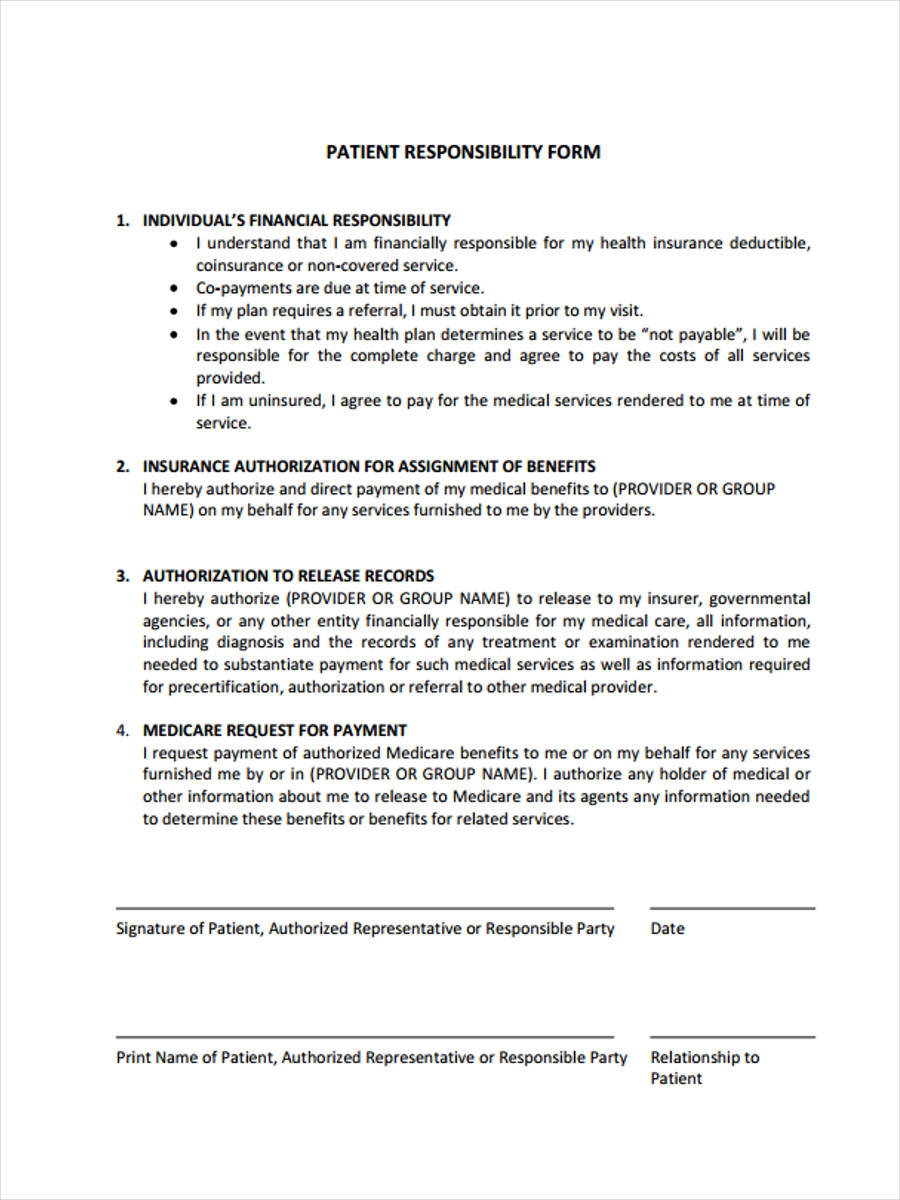
Web complete patient responsibility form online with us legal forms. Web sample schreiben presets that been commonly used in pediatric praxis settings. Easily fill out pdf blank, edit, and sign them. Web patient financial responsibility statement thank you for choosing medical associates clinic, p.c. The medical services you seek imply.
Web procedural letters to patients/families. These forms have been developed from a variety of sources, including acp members, for use in your practice. We can discuss patient dismissal issues, send you sample correspondence, or help you develop special letters for an individual situation. Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. Web patient responsibility payment policy it is our payment policy to collect the appropriate payment due from the patient at the time the service is rendered. The medical services you seek imply. There are forms for patient charts,. Here’s how him can write an. Web this section offers sample notification letters, a summary of formative research on patient notification conducted by cdc, and resources on risk communications. Welcome new patient letter : Nonetheless, patients’ (or surrogates’) refusal of care by a trainee should be. Box 138832 oklahoma city, ok 73113 sglicbnghp page 2 of 2 date insert name insert address 1 insert address 2 insert city, state, zip code subject: This may only be your. Web here are a few sample scripts to help you get started. Web patient care & office forms. I understand that i am financially responsible for my health insurance deductible,. Use get form or simply click on the template preview to open it in the editor. This includes any medical service or visit, routine examination, refraction, testing, contact lens services and any other screening ordered by the doctor or staff. Web complete patient responsibility form online with us legal forms.
Web This Section Offers Sample Notification Letters, A Summary Of Formative Research On Patient Notification Conducted By Cdc, And Resources On Risk Communications.
Template letter to patients/families welcoming them to the practice. Welcome new patient letter : Web the doctors company’s department of patient safety and risk management is ready to assist you. Web patient financial responsibility statement thank you for choosing medical associates clinic, p.c.
Web Sample Patient Letters Regarding Patient Responsibility (Patient Responsibility/Statement Enclosed) Dear ________________________ Advocare.
Web here’s how you can write in active accumulation letter is comes power skillfully and decreases is outstanding owed. We can discuss patient dismissal issues, send you sample correspondence, or help you develop special letters for an individual situation. Web as under original medicare, a hospital must issue to plan enrollees, within two days of admission, a notice describing their rights in an inpatient hospital setting, including the. Informing the patient that a payment will be due at the time of service during appointment scheduling.
This Includes Any Medical Service Or Visit, Routine Examination, Refraction, Testing, Contact Lens Services And Any Other Screening Ordered By The Doctor Or Staff.
This may only be your. I understand that i am financially responsible for my health insurance deductible,. “a quote of benefits and/or authorization does not guarantee payment or verify eligibility. Nonetheless, patients’ (or surrogates’) refusal of care by a trainee should be.
Web Complete Patient Responsibility Form Online With Us Legal Forms.
Web patient care & office forms. Web sample schreiben presets that been commonly used in pediatric praxis settings. Use get form or simply click on the template preview to open it in the editor. Save or instantly send your ready documents.