Medical Records Release Form Printable
Medical Records Release Form Printable - Web the information requested on this form is solicited under title 38 u.s.c. Pdffiller allows users to edit, sign, fill & share all type of documents online. Complete the attached form “authorization to use and disclose protected health information.” section 1 is asking you for. Use these forms when requesting transfer of your medical and billing records to or from another provider or to obtain a copy of your. Web allinahealth.org/medical records for a listing of allina health hospital and clinic locations and addresses. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Web to request a copy of your medical records: It also allows the added option for healthcare providers to share information. Web this arizona medical records release form is pretty brief, which only contains the sections of patient's name and date of birth, patient/guardian authorization, recipient's. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an.
FREE 12+ Sample Medical Records Release Forms in PDF MS Word Excel
Web medical and billing record release forms. Ad answer simple questions to make a medical records request on any device in minutes. You can use one of our free printable templates (pdf & word) to authorize the. Complete the attached form “authorization to use and disclose protected health information.” section 1 is asking you for. The form authorizes release of.
Medical Release Form Template Business
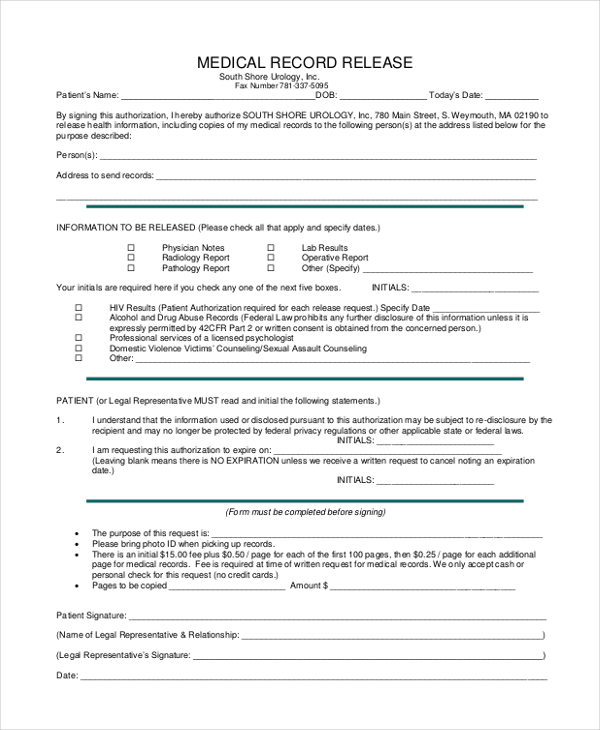
Complete the attached form “authorization to use and disclose protected health information.” section 1 is asking you for. The form authorizes release of information in accordance with the health insurance portability and. Ad answer simple questions to make a medical records request on any device in minutes. Send my medical records to: Web a consent form that includes a request.
FREE 10+ Medical Records Release Forms in PDF
Web form name:request for and authorization to release health information related to:health care form last updated:september 2022 when to use this form use. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Complete the attached form “authorization.
Medical Records Release Form templates free printable
(please print) last and first. Web you or someone you designate can access your electronic medical records from a computer or mobile phone from mayoclinic.org or the mayo clinic mobile app. Web to request a copy of your medical records: Web form name:request for and authorization to release health information related to:health care form last updated:september 2022 when to use.
Medical Records Release Form Templates at
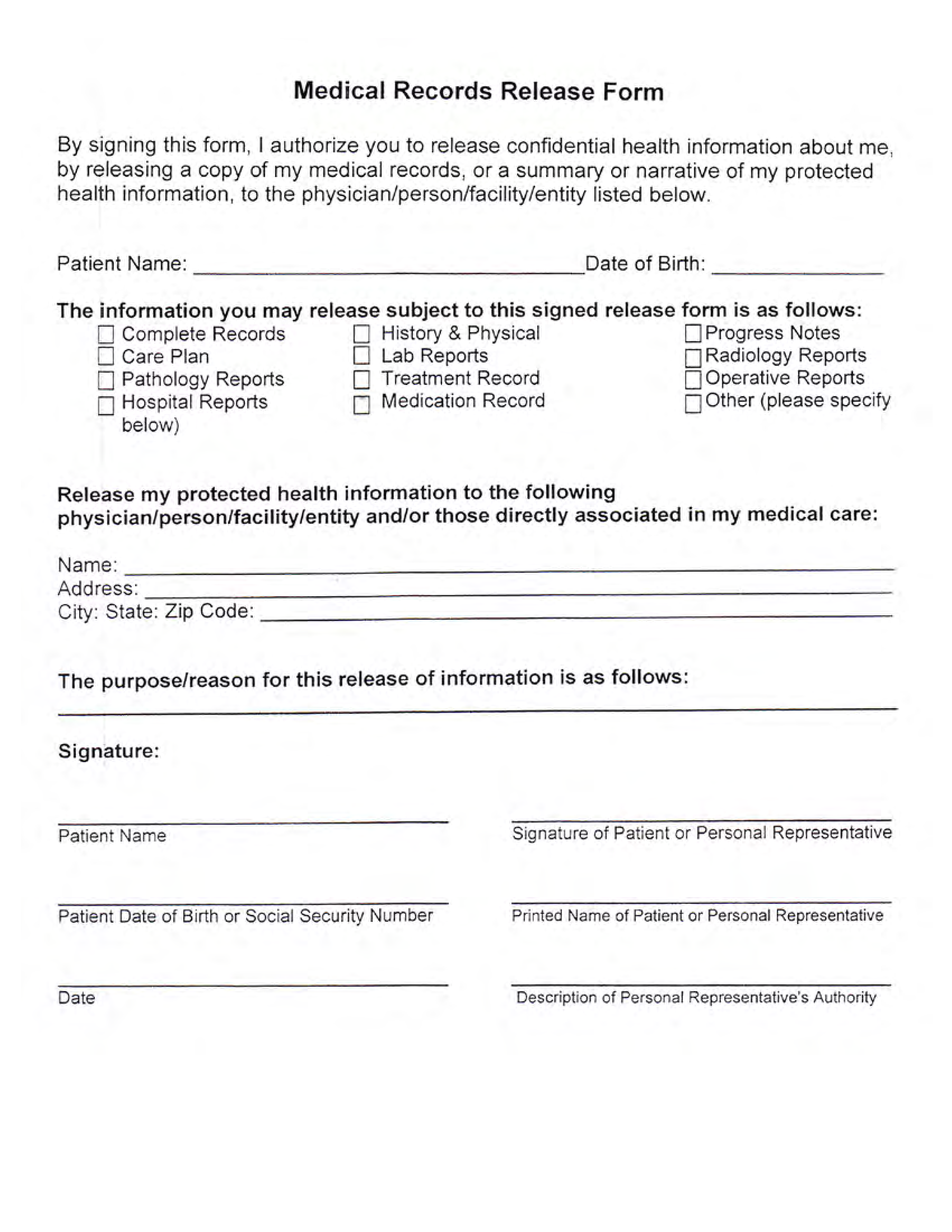
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. It also allows the added option for healthcare providers to share information. Web printed name of patient’s representative ____________________________________ date ____________________________________ relationship of patient this. A medical release.
Medical Records Release Form templates free printable
You can use one of our free printable templates (pdf & word) to authorize the. Web log in to your upmc patient portal account. Complete a medical records release form. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. The form authorizes release of information in accordance with.
FREE 9+ Sample Medical Records Release Forms in PDF MS Word
Pdffiller allows users to edit, sign, fill & share all type of documents online. Web complete and submit the appropriate authorization form below: The form authorizes release of information in accordance with the health insurance portability and. Web a consent form that includes a request for medical records is valid for 90 days from the date of signature. You can.
FREE 12+ Sample Medical Records Release Forms in PDF MS Word Excel
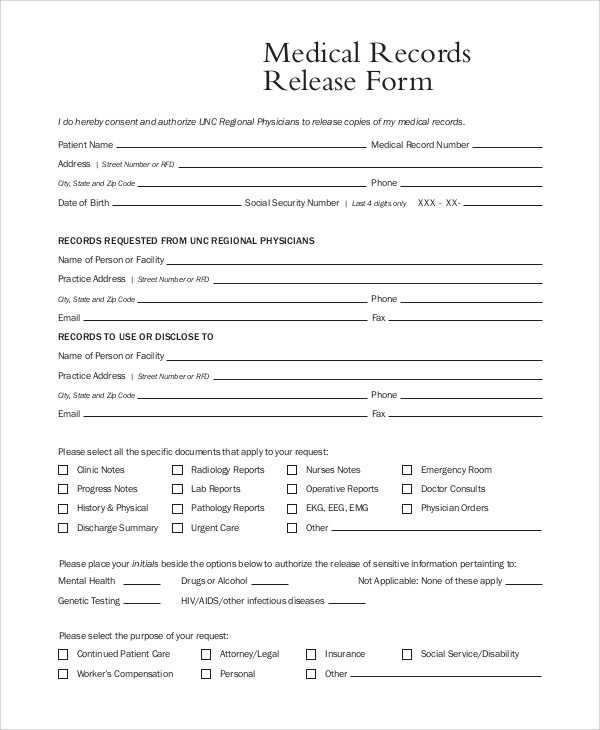
Web printed name of patient’s representative ____________________________________ date ____________________________________ relationship of patient this. If you don't have an account yet, learn how to sign up here. Web log in to your upmc patient portal account. Web please print all information clearly in order to process your request in a timely manner. Identify the full name/business, address,.

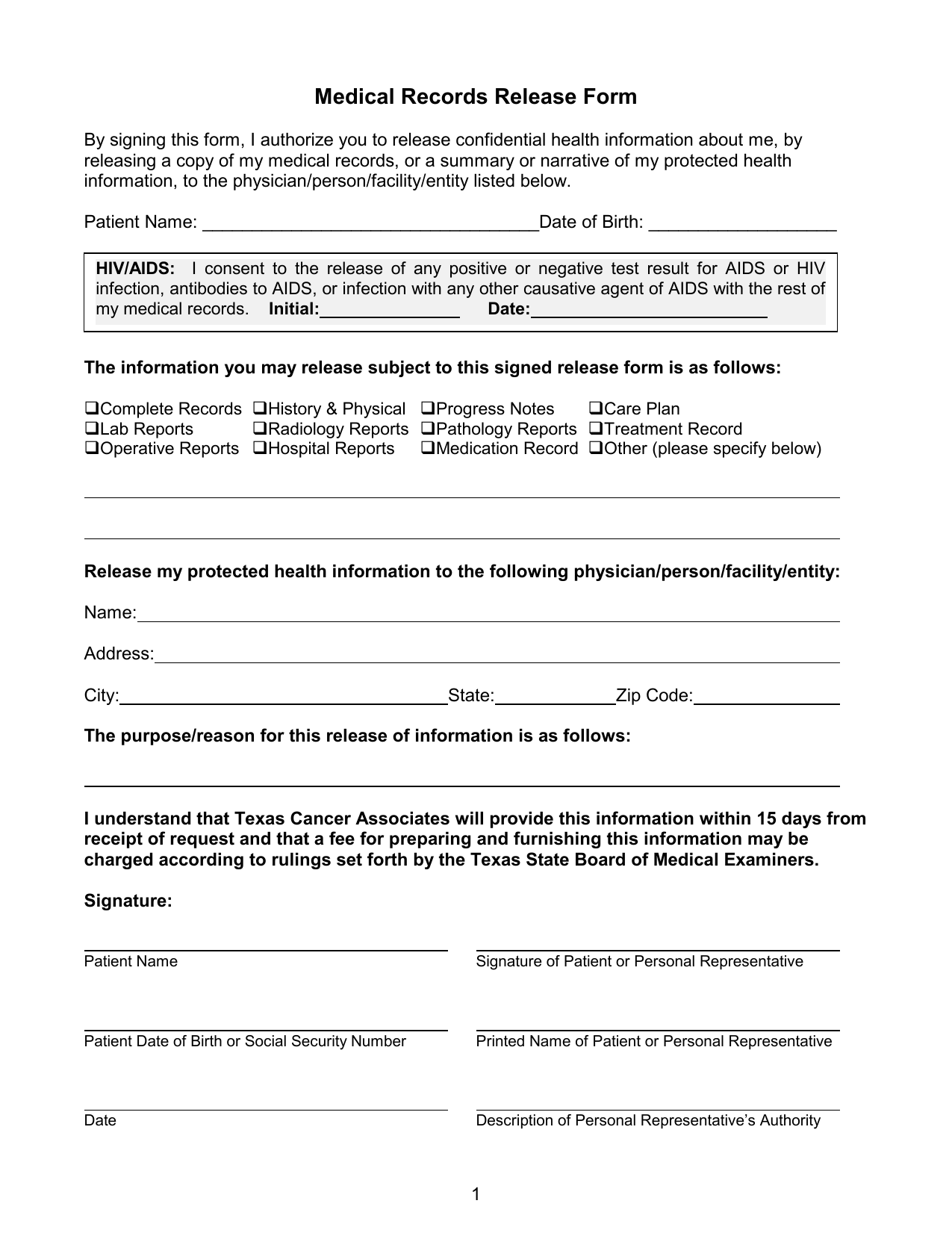
Texas Medical Records Release Form Download Free Printable Blank Legal
You can use one of our free printable templates (pdf & word) to authorize the. (please print) last and first. Web printed name of patient’s representative ____________________________________ date ____________________________________ relationship of patient this. Web authorization for release of information. Web a consent form that includes a request for medical records is valid for 90 days from the date of signature.
Medical Records Release Form Template Free Printable Templates
Web you or someone you designate can access your electronic medical records from a computer or mobile phone from mayoclinic.org or the mayo clinic mobile app. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. Pdffiller allows users to edit, sign, fill & share all type of documents.
You can use one of our free printable templates (pdf & word) to authorize the. Web please print all information clearly in order to process your request in a timely manner. Edit, sign and save medical release form. Web medical and billing record release forms. Web this arizona medical records release form is pretty brief, which only contains the sections of patient's name and date of birth, patient/guardian authorization, recipient's. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Identify the full name/business, address,. Federal law permits sources with information about you to release that information if you sign a single authorization to. Ad answer simple questions to make a medical records request on any device in minutes. The form authorizes release of information in accordance with the health insurance portability and. Web form name:request for and authorization to release health information related to:health care form last updated:september 2022 when to use this form use. Web you or someone you designate can access your electronic medical records from a computer or mobile phone from mayoclinic.org or the mayo clinic mobile app. Web to request a copy of your medical records: A medical release form can be revoked or reassigned at any time by the. Web the information requested on this form is solicited under title 38 u.s.c. Web a consent form that includes a request for medical records is valid for 90 days from the date of signature. Complete the attached form “authorization to use and disclose protected health information.” section 1 is asking you for. Web authorization for release of information. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. Web complete and submit the appropriate authorization form below:
Web Medical And Billing Record Release Forms.
Web the information requested on this form is solicited under title 38 u.s.c. If you don't have an account yet, learn how to sign up here. Pdffiller allows users to edit, sign, fill & share all type of documents online. The form authorizes release of information in accordance with the health insurance portability and.
(Please Print) Last And First.
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Web you or someone you designate can access your electronic medical records from a computer or mobile phone from mayoclinic.org or the mayo clinic mobile app. Complete a medical records release form. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records.
It Also Allows The Added Option For Healthcare Providers To Share Information.
Complete the attached form “authorization to use and disclose protected health information.” section 1 is asking you for. Authorization to disclose protected health information to family and friends adult patient. Send or bring the completed form to the subject of the record's local. You can use one of our free printable templates (pdf & word) to authorize the.
Medical Records Release Form Sample.
Web authorization for release of information. Web printed name of patient’s representative ____________________________________ date ____________________________________ relationship of patient this. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Web a consent form that includes a request for medical records is valid for 90 days from the date of signature.