Cms L564 Printable Form
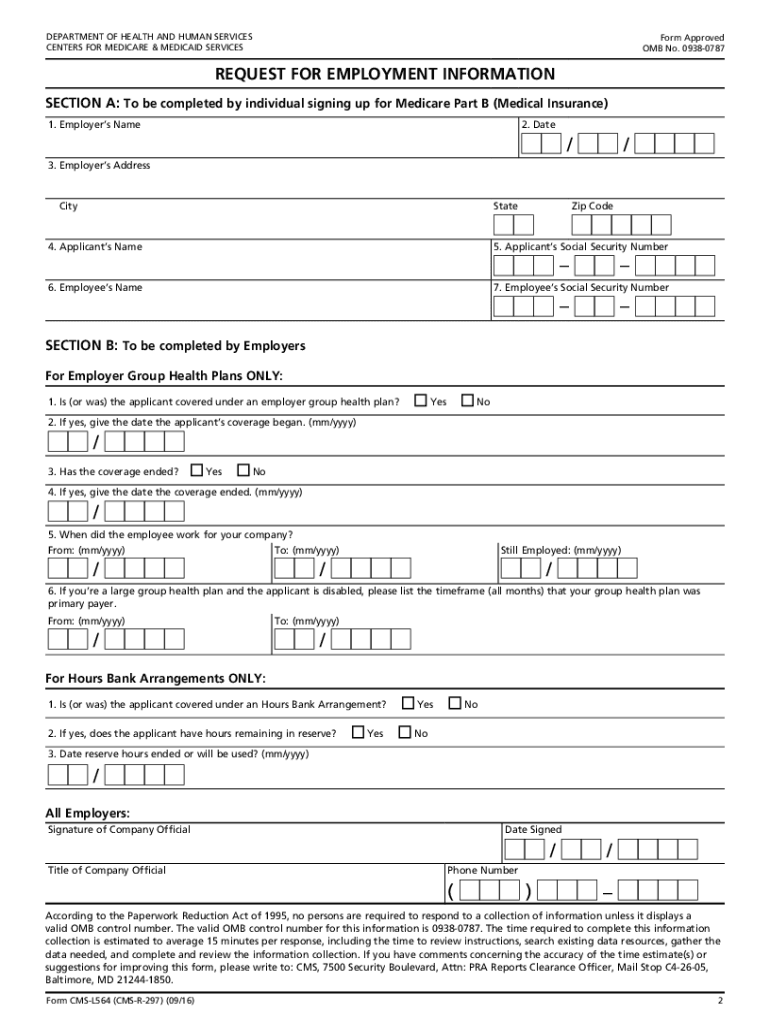
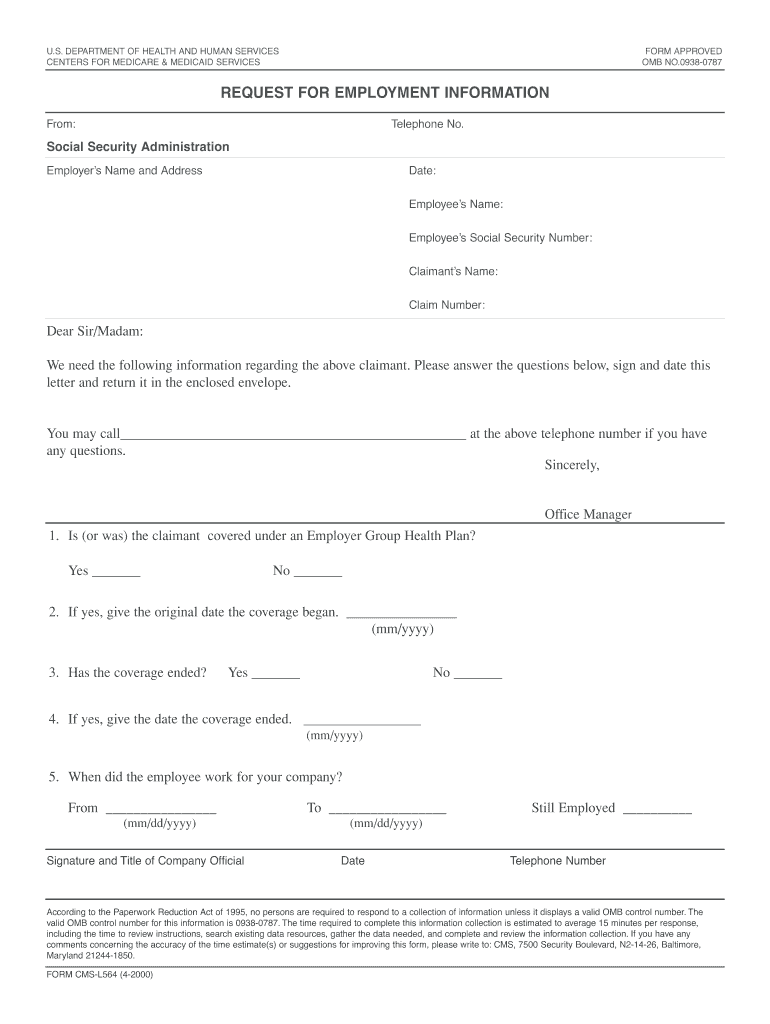
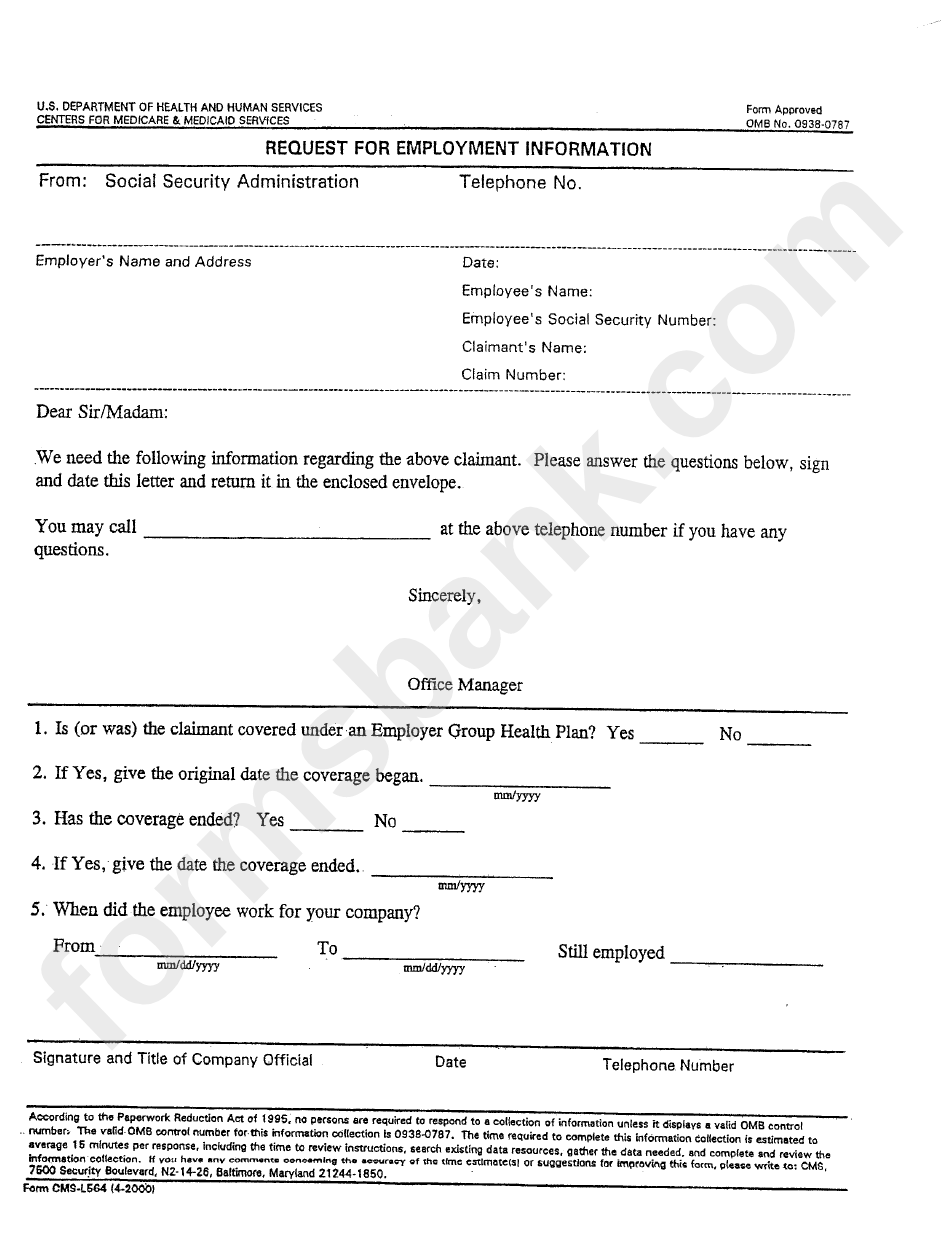
Cms L564 Printable Form - Web suggestions for improving this form, please write to: Save the completed cms l564. Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of your employment. Department of health and human services centers for medicare & medicaid services form approved omb no. In order to apply for medicare in a special enrollment period, you must have or had group health plan coverage within the last 8. This information is needed to process your medicare enrollment application. If you have a special situation, fill out the. You are responsible to fill out section a of this form with your employer’s name and address. Save or instantly send your ready documents. Try it for free now!
CMSL564 2016 Fill and Sign Printable Template Online US Legal Forms
Try it for free now! Upload, modify or create forms. Their spouses can join the plan. Easily fill out pdf blank, edit, and sign them. It is used only by those who have their plan covered by the entities where they work.

About Privacy Policy Copyright TOS Contact Sitemap
Send your completed and signed. Print the title of the company. It is used only by those who have their plan covered by the entities where they work. Web what is the purpose of this form? Cms, 7500 security boulevard, attn:
Form Cms L564 Form 20202022 Fill Out and Sign Printable PDF Template
Print the title of the company. Solicitud de información sobre el. Web what is the purpose of this form? Try it for free now! Upload, modify or create forms.

Form CMS L564 / R297 template
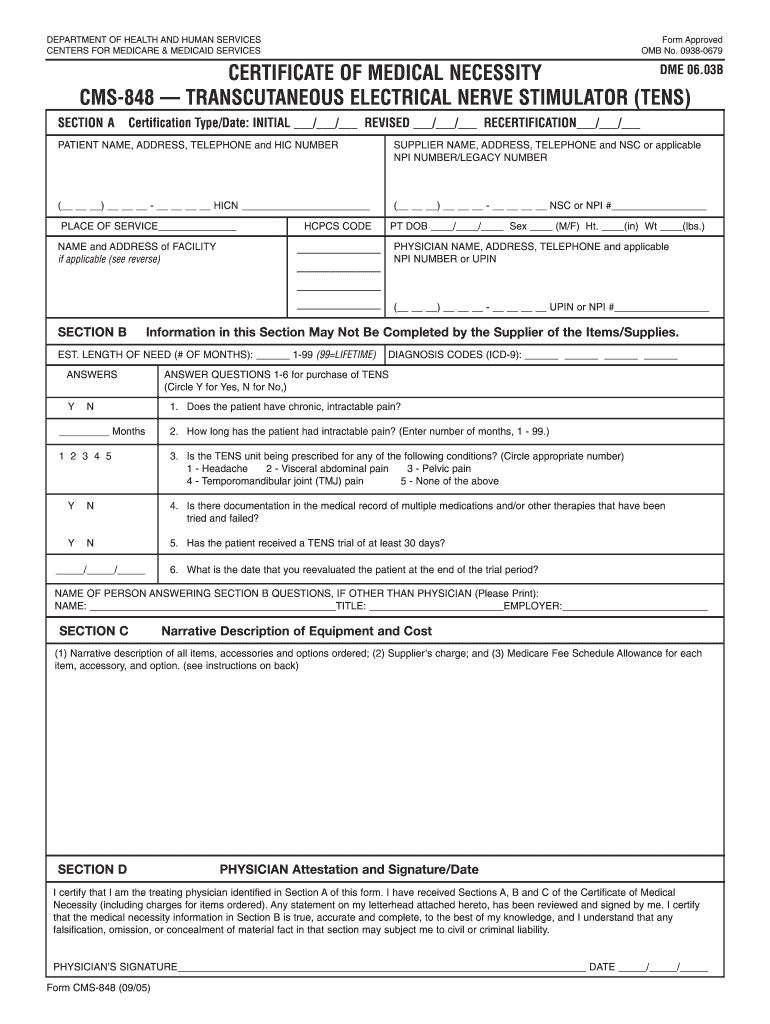
Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of your employment. Upload, modify or create forms. Web this form is used for proof of group health care coverage based on current employment. In order to apply for medicare in a special enrollment period, you must have or.
Medicare Part A Application Form Medicare Id Card Sample Inspirational
Print the title of the company. Cms, 7500 security boulevard, attn: Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of your employment. It is used only by those who have their plan covered by the entities where they work. Web suggestions for improving this form, please write.
Form CmsL564 Request For Employment Information printable pdf download
Web suggestions for improving this form, please write to: Print the title of the company. Upload, modify or create forms. In order to apply for medicare in a special enrollment period, you must have or had group health plan coverage within the last 8. Solicitud de información sobre el.
How To Fill Out Medicare Part B Application
If you have a special situation, fill out the. Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of your employment. Try it for free now! Try it for free now! Solicitud de información sobre el.

Medicare Part B Application Form Cms L564 Form Resume Examples
You are responsible to fill out section a of this form with your employer’s name and address. Web this form is used for proof of group health care coverage based on current employment. Try it for free now! Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of.

Gallery of Social Security Medicare form Cms L564 Awesome 54 Awesome
Cms, 7500 security boulevard, attn: This information is needed to process your medicare enrollment application. Upload, modify or create forms. Their spouses can join the plan. Solicitud de información sobre el.
Cms 84 fillable form Fill out & sign online DocHub
Open it up with online editor and begin altering. Save or instantly send your ready documents. Send your completed and signed. Web suggestions for improving this form, please write to: Cms, 7500 security boulevard, attn:
Web suggestions for improving this form, please write to: Web this form is used for proof of group health care coverage based on current employment. If you have a special situation, fill out the. It is used only by those who have their plan covered by the entities where they work. Open it up with online editor and begin altering. Try it for free now! Their spouses can join the plan. Send your completed and signed. Solicitud de información sobre el. Save or instantly send your ready documents. This information is needed to process your medicare enrollment application. Try it for free now! Cms, 7500 security boulevard, attn: Easily fill out pdf blank, edit, and sign them. You are responsible to fill out section a of this form with your employer’s name and address. Save the completed cms l564. Web fill out the cms l564 form with the required information, including your name, employer's name and address, and the dates of your employment. Department of health and human services centers for medicare & medicaid services form approved omb no. Upload, modify or create forms. Upload, modify or create forms.
If You Have A Special Situation, Fill Out The.
You are responsible to fill out section a of this form with your employer’s name and address. Upload, modify or create forms. Web suggestions for improving this form, please write to: Try it for free now!
Web Fill Out The Cms L564 Form With The Required Information, Including Your Name, Employer's Name And Address, And The Dates Of Your Employment.
Their spouses can join the plan. Easily fill out pdf blank, edit, and sign them. Web what is the purpose of this form? Department of health and human services centers for medicare & medicaid services form approved omb no.
Send Your Completed And Signed.
It is used only by those who have their plan covered by the entities where they work. Upload, modify or create forms. Save or instantly send your ready documents. Giving the social security administration proof you’re eligible to sign up for part b if:
Print The Title Of The Company.
Solicitud de información sobre el. Web this form is used for proof of group health care coverage based on current employment. Save the completed cms l564. If you’re signing up in a sep.