Chronic Care Management Consent Form Template
Chronic Care Management Consent Form Template - Patient consent agreement for chronic care management services. To qualify to bill for chronic care management services, the health provider must be classified as one of the following: 3) chroni c care management services 4) frequently asked questions about physician billing for chronic care management service s. Please consult your legal counsel. Discontinue this service at any time for any reason. Only one clinician can furnish and be paid for ccm services during a calendar month. A personalized care plan template to help patients take actions and meet their heath goals If another physician has offered to provide ccm, you will have to choose which physician is best able to treat and manage all your conditions. You have a right to: Web chronic care management services, so please ask my staff for the ccm revocation form.
Caregiver Daily Log Sheet Print Free Printable Caregiver Forms Free
Web get the chronic care management sample patient consent form you require. Chronic care management (ccm) consent. The goal of ccm is to help patients reachtheir health goals even when they are not in the office. You must sign an agreement to receive this type of chronic care management services. Web 1) cms chronic care management.

Medical Power Of Attorney For Child Pdf
Web this toolkit is designed to be used in two ways: Web cpt 99487 complex chronic care management services, with the following required elements: Web chronic care management consent. Web 1) cms chronic care management. Please consult your legal counsel.
Medical Consent Forms Template Collection
Web provide a personalized and comprehensive care plan management, easily shared to providers or family members; Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient chronic conditions place the patient at significant risk of death, acute exacerbation/ decompensation, or functional decline My physician, ___________________________________________ has recommended that. Fill out.

Elder Care Agreement (form 85) Form Resume Examples EVKYlD0106
Fill out the blank fields; A personalized care plan template to help patients take actions and meet their heath goals You authorize electronic communication of your medical information with other treating providers as part of coordination of your care. The clinician who is providing the primary care to the patient is the one who can bill. You have a right.

Printable Chronic Care Management Documentation Template Free Printable
You can only give ccm consent to one provider at a time. Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination form. Have the fooll wng ifive specified. You must sign an agreement to receive this type of chronic care management services. Web ccm consent form.
Information and Forms River Bend Medical Associates
During the visit, patients must sign a consent form to be initiated into the provider’s chronic care management program after which qualified clinical staffcan provide services to the patient remotely. The goal of ccm is to help patients reachtheir health goals even when they are not in the office. Concerned parties names, places of residence and phone numbers etc. Web.
Consent To Care And Treatment In Care Home Home Rulend
Core requirements needed to bill for ccm a. Web patient consent agreement for chronic care management services. Web chronic care management consent. Web cpt 99487 complex chronic care management services, with the following required elements: Patient consent agreement for chronic care management services.
Chronic Care Management Sample Patient Consent Form Fill and Sign
Web this toolkit is designed to be used in two ways: Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient chronic conditions place the patient at significant risk of death, acute exacerbation/ decompensation, or functional decline Web email chronic care management services (referred to as “ccm services”) are available.
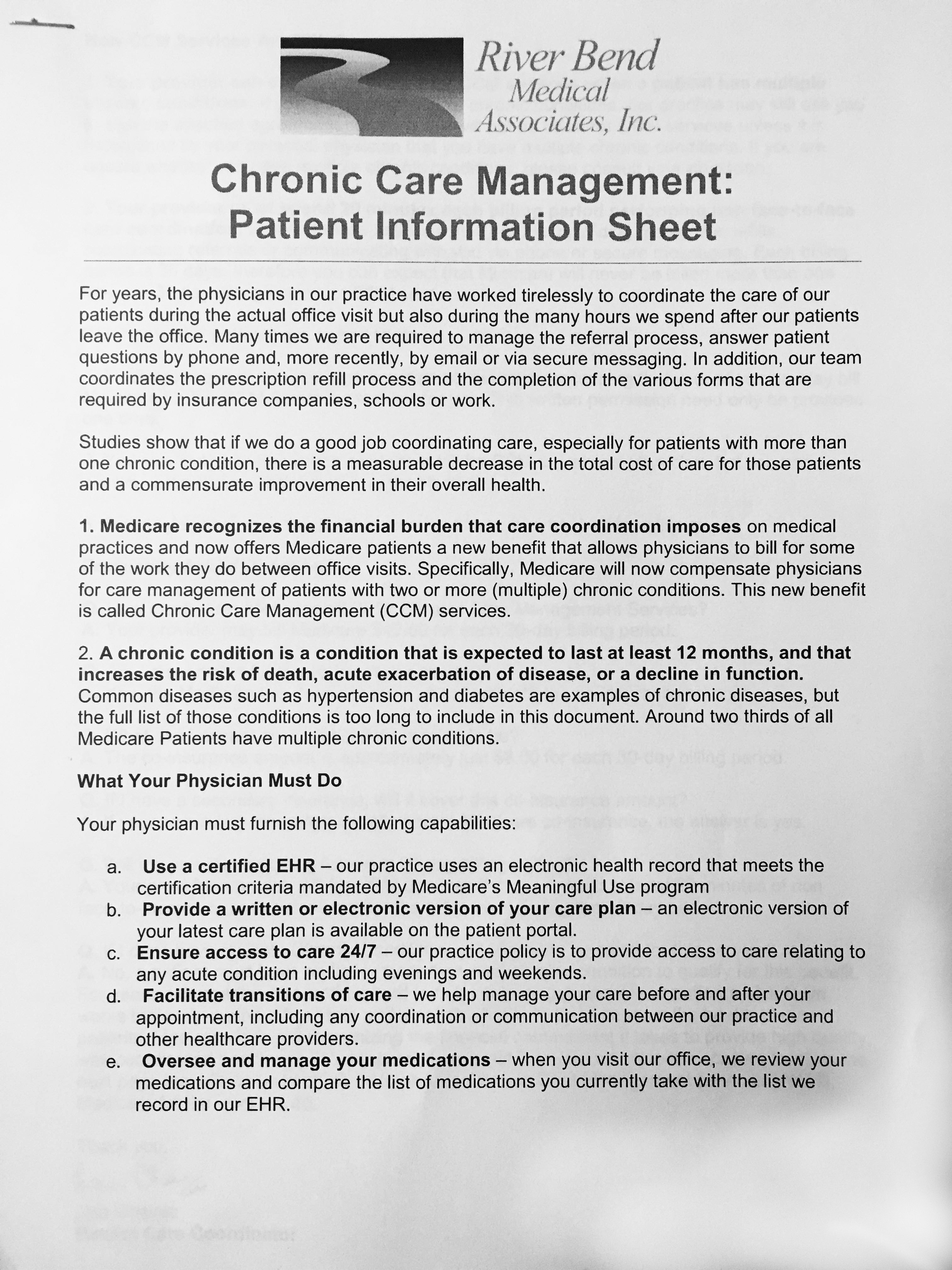
Information and Forms River Bend Medical Associates
As a resource for health care professionals to successfully build out ccm services in their practices and 2) as a tool to educate colleagues, members of professional societies, patients, and advocates about the importance of ccm in improving patient health and satisfaction. Discontinue this service at any time for any reason. Web 1) cms chronic care management. Core requirements needed.
Free Medical Consent Form The Five Secrets That You Shouldn’t Know
Web chronic care management consent. My physician, ___________________________________________ has recommended that. In alignment with our dedication to keep you as healthy as possible with a focus to keep you out of the hospital and minimize the costs and inconvenience of Care management such as variants of unknown significance and clinical trials reviewed monthly You have a right to:
Web cpt 99487 complex chronic care management services, with the following required elements: The clinician who is providing the primary care to the patient is the one who can bill. Web patient consent agreement for chronic care management services. Concerned parties names, places of residence and phone numbers etc. Care management such as variants of unknown significance and clinical trials reviewed monthly Patient consent agreement for chronic care management services. Web email chronic care management services (referred to as “ccm services”) are available to you because you have been diagnosed with two (2) or more chronic conditions which are expected to last at least twelve (12) months and which place you at significant risk of your healthcare declining. Web consent agreement for provision of chronic care management by signing this agreement, you consent to _______________________ (referred to as “provider”), providing chronic care management services (referred to as “ccm services”) to you as more fully described below. Web provide a personalized and comprehensive care plan management, easily shared to providers or family members; Web chronic care management services, so please ask my staff for the ccm revocation form. You consent to the provider providing ccm services to you. To qualify to bill for chronic care management services, the health provider must be classified as one of the following: Because your signature is required to end your chronic care management services, please ask any of our staff members for the ccm termination form. Web this toolkit is designed to be used in two ways: Please consult your legal counsel. During the visit, patients must sign a consent form to be initiated into the provider’s chronic care management program after which qualified clinical staffcan provide services to the patient remotely. In alignment with our dedication to keep you as healthy as possible with a focus to keep you out of the hospital and minimize the costs and inconvenience of Discontinue this service at any time for any reason. You have a right to: My physician, ___________________________________________ has recommended that.
You Can Only Give Ccm Consent To One Provider At A Time.
Web chronic care management consent form. Web ccm consent form for patients who agree to receive services; Have the fooll wng ifive specified. Only one clinician can furnish and be paid for ccm services during a calendar month.
Web Patient Consent Agreement For Chronic Care Management Services.
You have a right to: Chronic care management (ccm) consent. The goal of ccm is to help patients reachtheir health goals even when they are not in the office. Your provider believes that you would benefit from a chronic care management (ccm) program, a new medicare program for patients diagnosed with 2 or more chronic conditions expected to last at least 12 months and place your health at.
Ccm Is The Management Of These Chronic Conditions Outside Of The Regular Office Visits.
Your provider recommends you join a chronic care management program. You consent to the provider providing ccm services to you. Web get the chronic care management sample patient consent form you require. You authorize electronic communication of your medical information with other treating providers as part of coordination of your care.
A Personalized Care Plan Template To Help Patients Take Actions And Meet Their Heath Goals
Web by signing this agreement, you agree to the following: Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient chronic conditions place the patient at significant risk of death, acute exacerbation/ decompensation, or functional decline Web consent agreement for provision of chronic care management by signing this agreement, you consent to _______________________ (referred to as “provider”), providing chronic care management services (referred to as “ccm services”) to you as more fully described below. If another physician has offered to provide ccm, you will have to choose which physician is best able to treat and manage all your conditions.