Authorization To Release Information Template
Authorization To Release Information Template - Summary of agency confidentiality policy, circumstances. Web revoke your authorization and medicare will no longer give out your personal health information (except for the personal health information medicare has already given out. Web can revoke this authorization at any time by submitting a request in writing to ebd or filling out the authorization to revoke release of health information form. Web fill in the name, date of birth, and social security number of the subject of the record. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my. The specific uses and limitations of the types of. General release of information form word. Ad answer simple questions to make your information release. Web authorization to release information. Edit, sign and save uihc auth to bill insurance form.

Release Of Information Forms Printable (BLANK TEMPLATE)
Web revoke your authorization and medicare will no longer give out your personal health information (except for the personal health information medicare has already given out. General release of information form word. General services administration home reference forms. Web this document is a client authorization for releasing information to legal counsel. Summary of agency confidentiality policy, circumstances.
Free Authorization for Bank to Release Information Form PDF Template
At the request of the individual other: Web this document is a client authorization for releasing information to legal counsel. I authorize the testing facility , to release any and all medical information obtained during this exam and testing procedure to the (. I release and hold harmless the organization and its. Important elements for a release form include the.
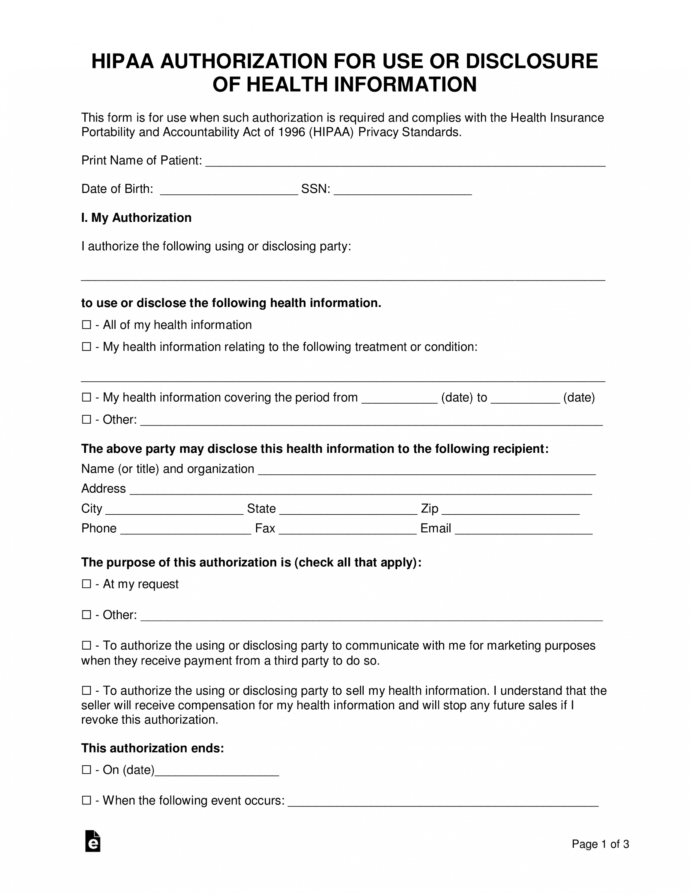
Free Free Medical Records Release Authorization Form Hipaa Mental
I authorize the testing facility , to release any and all medical information obtained during this exam and testing procedure to the (. Web revoke your authorization and medicare will no longer give out your personal health information (except for the personal health information medicare has already given out. At the request of the individual other: Web download this authorization.

Medical Information Release Authorization Form Template Addictionary
Web authorization for release of information | gsa an official website of the united states government u.s. Web download this authorization to release account information template design in word, google docs, apple pages format. Web i authorize the organization named above to release the following information regarding my employment with said organization. Web can revoke this authorization at any time.

Authorization to Release Information Download Printable PDF
General services administration home reference forms. Important elements for a release form include the following: Summary of agency confidentiality policy, circumstances. Fill in the name and address of the person or organization of where you want us to send the. At the request of the individual other:
Authorization To Release Information Template Template Business Format
Web i authorize the organization named above to release the following information regarding my employment with said organization. Web purpose for the disclosure: Providing this information is voluntary, but without it the department may find it more difficult to assist you in a manner consistent with your wishes. I authorize the testing facility , to release any and all medical.
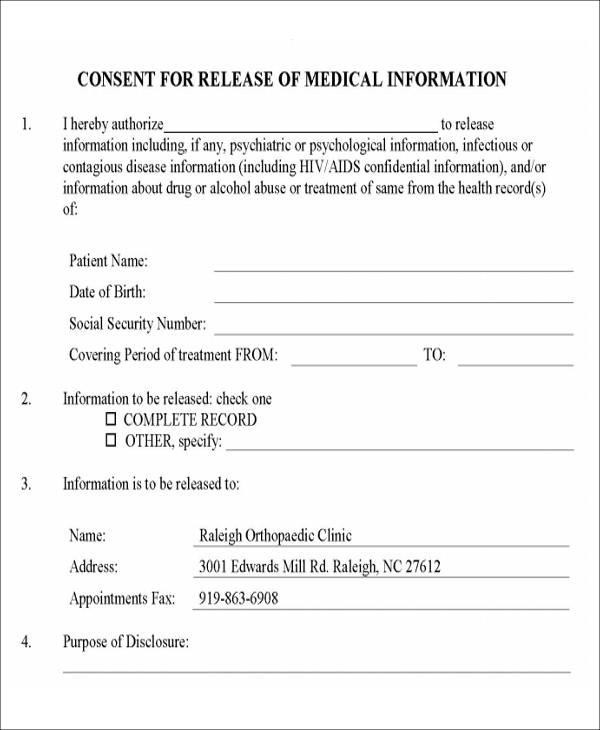
FREE 9+ Release Of Medical Information Form Samples in MS Word PDF
This consent form will expire on (date)_____________ or __________ days from the date of service recipient signature, whichever date comes. Web i authorize the organization named above to release the following information regarding my employment with said organization. At the request of the individual other: Web zip am requesting this disclosure of information and records for the following purpose: I.
FREE 13+ Sample Release of Information Forms in PDF MS Word
Web zip am requesting this disclosure of information and records for the following purpose: I authorize the testing facility , to release any and all medical information obtained during this exam and testing procedure to the (. Web release and /or exchange of information authorization. Ad answer simple questions to make your information release. Web authorization for release of information.
Authorization To Release Information Template Template Business Format
Web release and /or exchange of information authorization. Web authorization for release of information | gsa an official website of the united states government u.s. Ad answer simple questions to make your information release. Web fill in the name, date of birth, and social security number of the subject of the record. I authorize the testing facility , to release.
Authorization to Release Loan Information Fill and Sign Printable
At the request of the individual other: I authorize the testing facility , to release any and all medical information obtained during this exam and testing procedure to the (. Web authorization to release information. Web zip am requesting this disclosure of information and records for the following purpose: Web release and /or exchange of information authorization.
General services administration home reference forms. Edit, sign and save uihc auth to bill insurance form. Web can revoke this authorization at any time by submitting a request in writing to ebd or filling out the authorization to revoke release of health information form. Important elements for a release form include the following: Web download this authorization to release account information template design in word, google docs, apple pages format. The specific uses and limitations of the types of. General release of information form word. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my. Fill in the name and address of the person or organization of where you want us to send the. Web this document is a client authorization for releasing information to legal counsel. Web fill in the name, date of birth, and social security number of the subject of the record. At the request of the individual other: Providing this information is voluntary, but without it the department may find it more difficult to assist you in a manner consistent with your wishes. I release and hold harmless the organization and its. Web i authorize the organization named above to release the following information regarding my employment with said organization. Ad answer simple questions to make your information release. Web purpose for the disclosure: Web authorization to release information i/we hereby authorize you to release to _____ any and all information they may require for the purpose of a credit transaction, loan. Summary of agency confidentiality policy, circumstances. Web authorization for release of information | gsa an official website of the united states government u.s.
Web Authorization To Release Information I/We Hereby Authorize You To Release To _____ Any And All Information They May Require For The Purpose Of A Credit Transaction, Loan.
I release and hold harmless the organization and its. I authorize the testing facility , to release any and all medical information obtained during this exam and testing procedure to the (. Release of information template free. General services administration home reference forms.
Web Purpose For The Disclosure:
Web download this authorization to release account information template design in word, google docs, apple pages format. Web can revoke this authorization at any time by submitting a request in writing to ebd or filling out the authorization to revoke release of health information form. This consent form will expire on (date)_____________ or __________ days from the date of service recipient signature, whichever date comes. Web release and /or exchange of information authorization.
Summary Of Agency Confidentiality Policy, Circumstances.
Important elements for a release form include the following: Providing this information is voluntary, but without it the department may find it more difficult to assist you in a manner consistent with your wishes. Web zip am requesting this disclosure of information and records for the following purpose: Web printable blank authorization to release information form.
Web Revoke Your Authorization And Medicare Will No Longer Give Out Your Personal Health Information (Except For The Personal Health Information Medicare Has Already Given Out.
Ad answer simple questions to make your information release. Web authorization for release of information | gsa an official website of the united states government u.s. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my. Web i authorize the organization named above to release the following information regarding my employment with said organization.